World Voice Day
The annual "World Voice Day" takes place on April 16. This day was initiated in 1999 by ENT physicians, head neck and throat surgeons and speech therapists in order to draw attention to the extremely complex system of the human voice - but also to the diseases by which the human vocal organ may be affected.
In keeping with this year's motto "Lift Your Voice", we will take a closer look at this topic. The sound of the human voice is first generated right after birth as a reflex with the very first cry of the baby. Later on, the person learns to speak, form words and communicate with the aid of phonation. Whispering, jubilation, shouting, singing - all of this is possible with our voice. We use it constantly without consciously thinking about it.1 Only when hoarseness develops or we are affected by a more serious disorder do we become aware of how important it is to be able to express oneself vocally.
The function of the human voice
A person's voice is an individual feature by which we recognize each other and which also allows us to perceive emotional states. The human voice is actually a flow of air (energy supply) which is generated in the lungs, causes the vocal cords inside the larynx to vibrate and is then shaped acoustically as it passes through the throat and mouth. This vocal function is fundamentally changed for instance when laryngectomy surgery becomes necessary. In this procedure, the entire larynx is removed along with the vocal cords, so that at first, speaking is no longer possible at all. Complete separation of the trachea from the oesophagus is also functionally necessary in order to prevent constant choking when swallowing. Inhalation and exhalation then takes place exclusively via the tracheostoma.
Rehabilitation of the voice
The ability to communicate is a basic need that is vital for us. Voice rehabilitation is therefore an important priority after surgery. The aim of speech therapy is to find a replacement voice which is suitable for the person concerned. In order to be able once again to participate in social activities and regain one's normal social everyday life, it is helpful to relearn to speak.
There are a variety of alternatives that enable voice rehabilitation:
Pseudo-whispering
Pseudo-whispering is not only a form of vocal rehabilitation, but also at the same time provides the basis for learning two other vocal options (ructus voice or speaking with the electronic speech aid). In pseudo-whispering, the patient uses the air that is present in the oral cavity and over-articulates this through movements of the mouth.
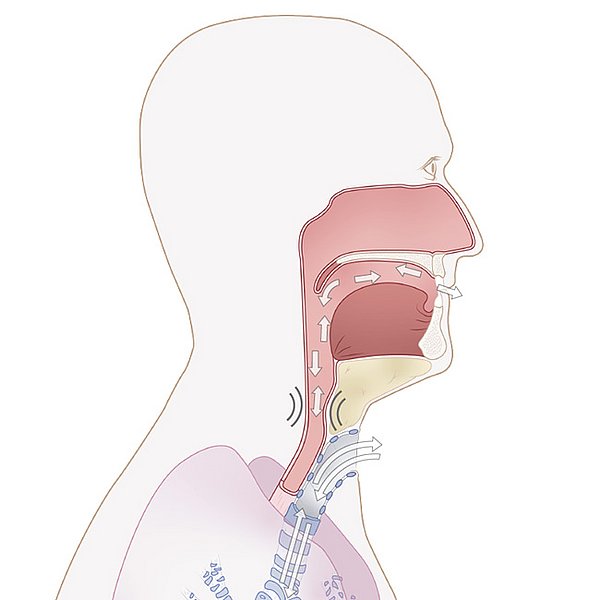
The ructus voice
In the ructus voice (oesophageal substitute voice), the air in the mouth is inhaled or pressed into the upper part of the oesophagus. This air remains there briefly and is then transferred back out of the oesophagus into the mouth in a controlled manner. This causes mucosal folds at the upper edge of the oesophagus to vibrate. This vibration creates a sound, which can then be articulated through movements of the mouth.
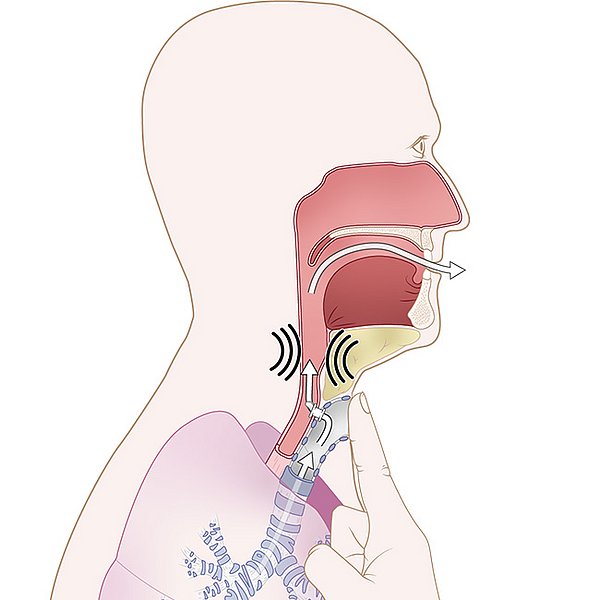
The voice prosthesis
The voice prosthesis (shunt valve) is a placeholder with a small valve, which is located between the trachea and the oesophagus in a so-called fistula channel. This valve is a one-way valve that prevents food and liquids from passing from the oesophagus into the trachea. When handled correctly, e.g. by manual closure of the tracheostoma, this valve allows air to enter the oesophagus during exhalation. As with the ructus voice, the "vocal segment" there is made to vibrate to create a sound. This sound can then be articulated and used for speaking. With this substitute voice, the long duration of utterance is a great advantage, as the entire volume of exhaled air can be used for speaking. The voice prosthesis is inserted either in the course of primary surgery for laryngectomy, or in the course of another, later surgical intervention.
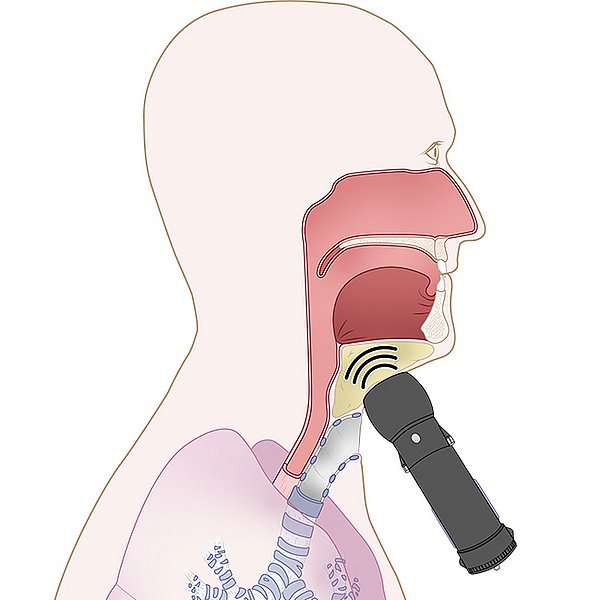
The electronic speech aid
This method employs an electronic device to produce sounds for speaking. The device is held against the cheek, chin or neck, where it generates sound vibrations which are transmitted to the air in the mouth and throat, where they can be used for speaking. Once a suitable contact point has been found on the soft parts of the neck for the device, learning this substitute voice is possible quite quickly and without complications. In the course of speech therapy, the length of utterance, intonations and handling of the device are practised and adjusted on an individual basis. The electronic speech aid requires pseudo-whispering as prerequisite.
Conclusion
Voice rehabilitation after laryngectomy is a very complex matter. It already commences at the intraoperative stage as appropriate for the tumour-related situation and is then continued on a professional level in the scope of speech therapy. The aim is to find a concept to fit the patient's individual needs.
The medical aids and therapy best suited for the individual patient are therefore coordinated appropriately in a close cooperation of speech therapists, physicians and providers of medical aids,.


